By Carissa Wong, PhD Cancer Immunology
November 18-24th is World Antibiotics Awareness Week; here, a look at how economics fundamentally shapes resistance research efforts.
A recent review published in Science highlights the parallels of climate change and antimicrobial resistance (AMR); both are global crises which require international intervention. Without appropriate solutions, these issues will be massive costs to human life and the global economy.
Reports commissioned by the UK government have forecast that, globally, 10 million annual deaths, a GDP reduction between 2 to 3.5 percent and a cost of $100 trillion could result by 2050 if we do not tackle AMR appropriately. Such challenges must be dealt with by policymakers, and the economic landscape is the strongest force guiding their search for solutions. Here we look at the economics of AMR, and what needs to be done to avert a world where a small scratch could prove fatal.
Penicillin was the first antibiotic to be discovered by Alexander Fleming in 1928, before development as a medicine by Ernst Chain and Howard Florey. The power of antibiotics to transform healthcare was officially recognised when they jointly received a Nobel Prize in 1945; even then, they warned that bacteria could become resistant to antibiotics via natural selection.
Today, modern medicine relies on antibiotics to mitigate the dangers of procedures common in high-income countries (HICs) such as caesarean sections, chemotherapy and joint replacements. In a world where AMR is more common, there will be higher rates of disease, more complications and longer hospital-stays; this will cost time, lives and a lot of money.

As with climate change, the impact of AMR on the world will not be evenly distributed. For low-and-middle-income countries (LMICs) the effects of AMR are likely to be worse than for HICs. Hospital infection control systems are often worse in LMICs. Moreover, AMR and climate change are likely to increase poverty within countries. For example, the productivity of people in lower-income agricultural work will be severely impacted by the climate and their physical health.
The future of AMR is uncertain. It is incredibly difficult to predict how and when AMR will develop, because new resistance genes can be quickly spread across bacterial populations at any time or in any place. It would be best to assume the worst-case scenario will occur and have insurance policies in place, given the enormous costs involved. However, this uncertainty also provides politicians, who prioritise short-term gains, with reasons to ignore the long-term threat of AMR - as has been the case with climate change.
We need multiple antibiotics to treat a given infection, so that fewer will become ineffective if the bacteria acquire a certain resistance gene. However, there is a lack of incentive to create new antibiotics. Pharmaceutical companies have little reason to invest in the development of new antibiotics because clinical trials are expensive, logistically difficult to conduct, and any new antibiotics must be limited for use to reduce the rate of resistance developing.
Once the antibiotic is in use, the development of AMR will reduce its value. Producing new antibiotics is unlikely to be profitable, especially when many candidate drugs fail to successfully pass through the stages of development. Novartis recently followed in the footsteps of many pharmaceutical companies when it stopped investing in antibiotic research in 2018.
The current system for producing antibiotics means profits are determined by the cost of the antibiotics and the amount sold; this system makes fighting AMR a losing battle. New approaches are required such as providing more funding support for companies to develop antibiotics, or ensuring companies profit from antibiotic-development research by providing a guaranteed financial gain independent of the extent of sales.
Inappropriate usage of antibiotics, which drives AMR, may result from misdiagnoses by doctors, financial motives for doctors in places where prescribing and dispensing antibiotics are not separated, and patients not completing their prescribed course. Overprescribing could be avoided by improved diagnostic tests that more accurately pinpoint the cause of disease.
Ensuring doctors cannot financially gain from increased prescription of antibiotics will prevent conflicts of interest that encourage AMR. Improved education on how AMR develops is of utmost importance, as many are not fully aware of the consequences of misuse. This will also help to reduce the pressure doctors can be placed under by patients to inappropriately prescribe antibiotics.
The international 2015 Paris agreement to combat climate change would not exist without informative economic analyses. Economics equally has a role in developing solutions for AMR. While climate change has over 16,000 peer-reviewed articles published in the economic EconLit database, there are only 55 about AMR. Tackling AMR through an economic lens is an approach that must be used to solve the crisis and we can learn a lot from the campaign against climate change.
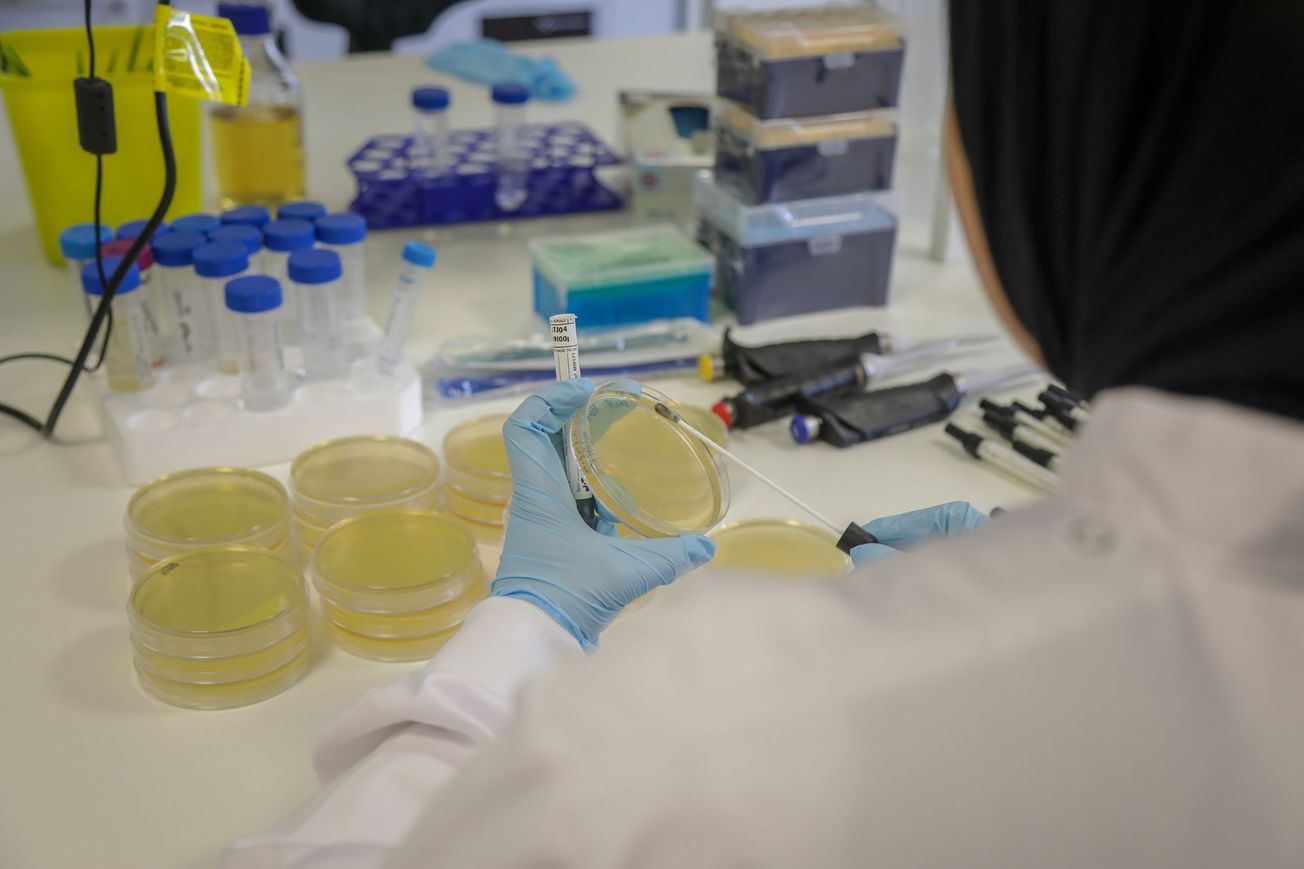
Featured image: Flickr / DFID
Concerned about antibiotic resistance? Get in touch!






{kind=link}